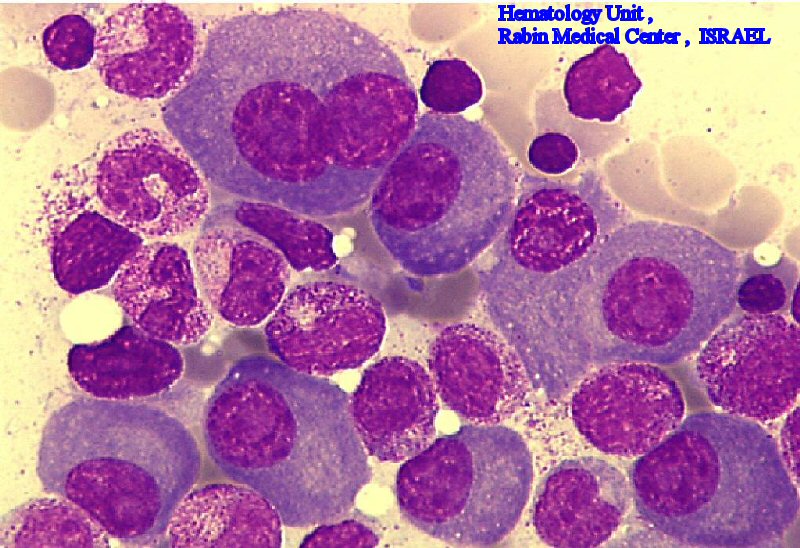
Bone marrow biopsy demonstrating sheets of malignant plasma cells in multiple myeloma

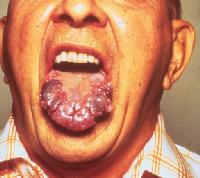
Amyloidosis infiltrating the tongue in multiple myeloma
Radiograph of the skull demonstrating a typical lytic lesion in multiple myeloma

Yeah, Its Wednesday and I have nothing better to do than study Plasma Cell Disorders. He is at work so I cannot even talk to him. I already called him like 4 times to talk to him but No ANSWER!!!! But, at least I am getting something done. I am at home racing through these lectures. I am definitely going to have to workout today. Get 200 calories burned on the treadmill. So I weigh 125lbs and I used to weigh 110lbs. That's a lot of pounds to lose. I have become a "Food Lover" and at times obsessive. But then again, I don't eat that much. I think I just need to trim the fat away by running more. What do you all think?
PLASMA CELL DISORDERS:
--> MULTIPLE MYELOMA(MM):
- overproduction of abnormal plasma cells
- 3 primary disease processes: expanding plasma cell mass, overproduction of monoclonal immunoglobulins, & production of OAF and cytokines (IL9)
- effects of monoclonal gammopathy: hyperviscosity syndrome, bence-jones proteins, amyloidosis
- effects of Osteoclast Activating Factor (OAF) and cytokines: bone destruction, lytic lesions, hypercalcemia
- BM biopsy: taken @ 2 different sites, usually >10% plasma cells (min) & >30% (max) seen in MM
- Protein Electrophoresis: indicates a presence of monoclonal spike
- Immunoelectrophoresis: specifies the type of monoclonal spike (ex: IgM or IgG)
- Chemistry tests: BUN and Creatinie for kidney function (should be high), LDH is high, Calcium is high, uric acid is high, albumin is low
- 2 reliable markers of MM: Beta1 microglobulin & C-Reactive Protein
--> SMOLDERING MYELOMA:
- Low mass MM
- Normal kidney function, serum calcium
- No lytic bone lesions
-->SOLITARY PLASMOCYTOMA:
- Single tumor found outside the BM
- BM contains <10%>
- treatment: radiation therapy
-->PLASMA CELL LEUKEMIA:
- rare, presence of significant number of plasma cells in peripheral blood (PB)
- >20% plasma cells in the differential
- less bone pain than MM, organ infiltration is excessive, no hyperviscosity syndrome
- low hgb/hct; leukocytosis; thrombocytopenia; rouleax; high BUN and creatinine
-->MONOCLONAL GAMMOPATHY OF UNDETERMINED SIGNIFICANCE (MGUS):
- small M-spike on serum protein electrophoresis
- small amount of urine light chains
- no lytic bone lesions
- <10%>
-->WALDENSTROM'S MACROGLOBULINEMIA (WM):
- overproduction of monoclonal IgM antibodies by cells called plasmacytoid lymphocytes
- fatigue, weakness, weight loss, plasmacytoid lymphocytes infiltrate nerves, meninges, and brain
- prominent feature: hyperviscosity syndrome (retinopathy)
- cryoglobulins: IgM that precipitate on exposure to cold; bleeding form gums and nose; cryoglobulinemic purpura; abnormal coagulation tests,raynaud's phenomena
- no cure; chemo + plasmaphoresis
-->HEAVY CHAIN DISEASE:
- very rare
- excessive production of heavy chain portion of antibody unit
- plasma cells have lost the ability to synthesize the light chain component
- so far IgG, IgA, IGM cases have been reported
1 comment:
thanks guys....Platiejo, I can never get on your link because it doesn't work for some reason.
Post a Comment